 |
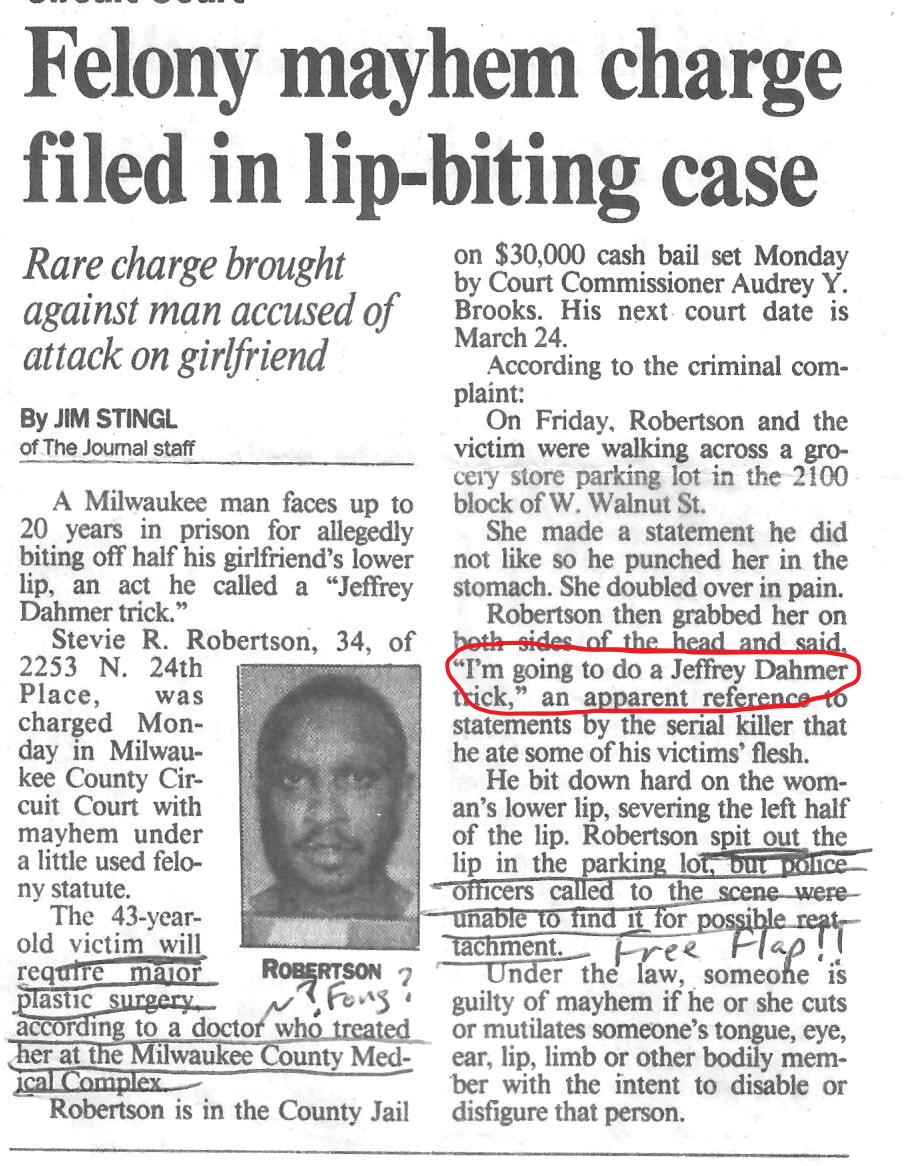
| Article from The Milwaukee Journal, March 1992 |
Halloween is a-coming, which brings to mind a personal story of decapitated heads.
One day in March
1992 as the ENT resident on-call, I was summoned to the emergency room for a
poor woman who lost a large portion of her lower lip. A victim of domestic violence, she said her
boyfriend punched her in the stomach in a parking lot. When she bent over in pain, he grapped both
sides of her head and said, “I’m going to do a Jeffrey Dahmer trick,” as he bit
a large chunk of her lower lip and spit it out.
As a first-year
ENT resident, I was at a loss for what to do.
The police who later arrived at the scene could not find the lost lip. So there she was in the ER with a large
gaping wound exposing some of her lower teeth, no tissue to reattach, and a
newbie resident scratching his head (figuratively of course). I called the senior resident who advised me
to clean the wound, admit her and start her on i.v. antibiotics (human bites
can cause hideous infections), and we’d later find a
way to reconstruct it (with an advancement flap or a “V”-shaped wedge excision,
a techique used for lip cancersm followed by closing the wound in straight-line
fashion). I explained the plan and reassured
her we could repair this as I dressed the wound and admitted her to the
hospital.
The following day
the story appeared in The Milwaukee Journal, one of Wisconsin’s major
newspapers. The
reporter included much of the above story along with the Jeffrey Dahmer
reference but also added, “…victim will require major plastic surgery
according to a doctor (me) who treated her at the Milwaukee County Medical
Complex.” I didn’t exactly say those
words, but the senior resident, who clipped out the article, and the other
residents on the team had a merry jokefest at my expense.
*
* *
That prior summer
in July 1991, the notorious serial killer, Jeffrey Dahmer was caught and
arrested right there in Milwaukee. In
one of the most twisted mass-murder stories, his killing spray started over a
decade and a half before, ultimately murdering 17 people in his lifetime. His last victims were in Wisconsin. Upon his arrest, police soon found seven
decapitated heads in his Milwaukee apartment, not far from the Medical College
of Wisconsin (the unofficial acronym is MCOW) and the county medical
complex where we trained.
*
* *
Talk of
disembodied heads has a significance beyond recanting a gory story in
Milwaukee; it is relevant to doctor-traiing beyond the unique ER experience for
one green resident. Each year we ENT
residents moseyed down to the gross anatomy lab at MCOW, that same place where
I first encountered a cadaver. Only this
time, the cadavers had been fully dissected, the gross anatomy class had
concluded for the year, and the med students no longer needed them. Prior to the planned cremation of the
remains, we harvested temporal bones—the hard bone on each side of the skull
housing the ear and all of its complex inner structures. Bringing dissection instruments including
bone saws, we worked away on a Saturday morning cutting and sawing, sometimes
with music playing in the background or humming the Wizard of Oz tune, “If
I only had a brain...”
There is an
educational purpose for all of this. Our
residency program had a lab devoted to temporal bone dissection. The lab was equipped with high-speed drills
designed for bone removal, fine surgical instruments, operating microscopes
mounted on the bench-tops, and specialized metal devices designed to secure the
temporal bone as we performed a mastoidectomy or a variety of ear surgeries,
simulating what we’d actually do in surgery.
When time permitted, a few of us would meet in the lab on a Saturday or
Sunday to practice these skills.
Occasionally we’d
have fresh cadevers for other surgical procedures. In one hospital, I was encouraged to
periodically visit the morgue and ask for permission to perform sinus
surgery. One day the pathologist stated
he had a body, family consented to have it used for study prior to
cremation. On a Saturday I rolled the
large tower containing the endoscopic and video equipment down to the
morgue. The Attending who encouraged me
to do this also advised that while practicing the routine endoscopic procedures,
I should also deliberately violate surgical boundaries; namely, do the things
we weren’t suppose to do in real-life that lead to complications, such as
dissecting through the skull base into brain or into the orbit containing the
eye. Surgical dissection on fresh tissue
comes as close to live surgery, except for the absence of blood, which perhaps creates
the most difficulty in actual surgery. Yet
actual human tissue is far superior than anatomic models made of artificial
materials and is enormously beneficial for developng proper surgical skills and
appreciating the nuances of anatomy that cannot be fully understood from
textbooks or other simulated media. Of
course, most of our surgical skills came from operating on real patients under
he auspices our attendings.
Fresh heads were also valuable for the instruction
of otolaryngologists already in practice, long after completing their
residencies, especially for those who needed training in the newer endoscopic
techniques (which nowadays are standard for sinus surgery). Our chairman was one of several
nationally reknowned academic otolaryngologists who toured the country teaching
these newer techniques. When the course
was offered at MCOW, the residents were responsible for harvesting fresh heads
from the morgue, and we stored them in a refrigerator in our temporal bone lab,
eventually bringing them to one of the anatomy labs at the medical school for
the weekend course. As a “reward,” we
residents were given one of the heads for our practice. Endoscopes, surgical instruments and video
monitors for each head were part of the course package, as the instructors
guided the attendants through the proper surgical techniques.
Thoughts of Dahmer still trigger a queasy feeling even when I reflect upon it years later; the passage of time has not quelled my uneasy mind about that history. And yet working on a cold head back in those days as a young resident did not elicit that same visceral reaction, and Dahmer rarely crossed my mind during those times. This is yet another example of the mindset employed during medical education, where detachment naturally arises while deeply absorbed in worthwile work and study, all for a greater purpose..
©Randall
S. Fong, M.D.
For more topics on
medicine, health and the weirdness of life in general, check out the rest of
the blog site at randallfong.blogspot.com
Comments
Post a Comment