
See that instrument above?
Look menacing? You may ask, “Does
it hurt? Is my doctor a masochist? Or is he merely a lunatic?” Thoughtful questions we’ll answer in a
minute.
One day you’re sitting in the ENT doctor’s exam room,
reading the latest viral You-Tube video on your cell phone (despite ignoring
the signs everywhere instructing you to silence and put your cell away) when
the doc gleefully enters the room. He
introduces himself, but you raise your finger as a signal to pause, that you’re
in the middle of an entertaining video that you simply must finish. After completion, you finally look up at the
doc, who is turning to leave the room to see another patient. You yell something like, “Hey! Where ya going?” and the doc turns back
around. He reintroduces himself since
you weren’t paying attention the first time and asks what brings you to the
office.
You declare that you don’t have a problem, but your spouse,
friends, coworkers, even your mother, all complain about your hearing. You clarify that your hearing is fine--it’s
everyone else who has the problem. Either
they’re speaking too softly or enunciating poorly. After repeating things to you over and over
again, they shake their heads in frustration and yell at the top of the lungs, demanding
you see a doctor.
“So doc, what’s wrong with those annoying people?” you ask the
bewildered doctor. Just then you hear a
ping on your cell and it’s a must-see text message with a video of two adorable
kittens riding atop a German Shephard chasing a frazzled coyote. After putting your cell back down, you stare
at your doctor.
“So what gives doc?
You haven’t answered my question.”
The doc looks perplexed and perhaps annoyed, and after
rudely suggesting you should not turn to your cell every time it makes a noise,
you agree to allow further history-taking and the performance of a physical
exam, despite all the rings and pings spewing forth from your beloved phone. You have a burning desire to pull out your
cell, but the doc is doing all sorts of weird things like talking to you,
examining you, even looking into your ears.
This is all semi-acceptable to a point, but then out comes this whacked-out
device. You’d swear it’s an instrument
for torture, payment for your disrespectful cell phone use. At that moment, you wish you’d purchased that
Tazor attachment for your phone. You
feel defenseless.
O.K., the tuning fork looks a little creepy. It has the shape of a blunt serving
fork. Whenever I bring this out and
strike it on my elbow to activate it, some folks respond with a look of horror
and back away in the exam chair. A few
kids had jumped out the chair and ran to Mom or Dad or headed for the exit.
Anyway, after explaining I won’t strike their head with the fork
or put it onto some other unmentionable body part, that it merely vibrates
which feels kinda funny but is painless, most people allow me to proceed,
though there’s a doubtful expression, an uncertainty of whether I’m still a
creepy dude.
There are various sizes of tuning forks, each vibrates at a
specific frequency. Once activated by
striking the fork on a hard surface such as the edge of a counter or table (I
use my elbow, which sometimes hurts, but I’m all for suffering for the patient)
sound is generated by the movement of air molecules in wave-like fashion from the
fork. Check out the prior article Hearing
and The Physics of Sound Mechanics for more glorious detail on the
working mechanics of sound.
Sound waves must travel into the ear canal and vibrate the
tympanic membrane (abbreviated TM) and the small bones (ossicles) attached to
it. Collectively, the TM and ossicles
are part of the middle ear.
Afterwards, a bunch of cool processes occur within the inner ear
(cochlea) that eventually convert sound energy into electrical signals that travel
along the auditory nerve to your brain, where the sound input is further
processed into meaningful information.
See Hearing
and How the Ear Processes Sound for more discussion on how the ear
processes sound.
The tuning fork is a nifty device that can provide a lot of
information about one’s hearing problem if more elaborate equipment is not
readily available (i.e., a fancy, expensive audiometer and a steel-encased,
soundproof audio booth). But before we
get into the features of the fork, I’ll briefly touch upon the different types
of hearing loss.
TYPES OF HEARING LOSS
Conductive hearing loss (CHL): this arises when there is a problem in the middle
ear, the part of the ear that includes the tympanic membrane and the
ossicles attached to it. Sound is conducted
along these small but moveable thingamajigs to the cochlea. Examples of problems causing CHL are a
tympanic membrane perforation (hole in the TM), otitis media (where there is
pus or fluid in the middle ear behind the TM), stiffness of the ossicles (otosclerosis
is an example) to mention but a few.
Sensorineural hearing loss (SNHL): The cochlea is the snail-shaped sensory organ that
ultimately receives input from the TM and ossicles. It is connected to the brain by the auditory
nerve. Hearing loss due to a problem
with either the cochlea or the auditory nerve is termed sensorineural
hearing loss, since it is often difficult to determine whether the cochlea or
the nerve or both are affected. One of
the most common causes of SNHL is loud noise exposure. SNHL also often occurs as a normal decline of
hearing with aging, known as presbycusis.
Mixed hearing loss (MHL): This arises when both a conductive AND a
sensorineural hearing loss is present.
For instance, a hole in the tympanic membrane in a patient with
noise-induced SNHL will create a mixed loss, or an elderly patient (with
presbycusis, or age-related SNHL) with otitis media (fluid behind the TM). In both examples, the defect in middle ear prevents
proper conduction of sound from the TM down the ossicular chain creating the
CHL. The defective cochlea or nerve from
prior noise injury or aging creates the SNHL.
The tuning fork can help determine the presence of hearing
loss and often the type of hearing loss.
TUNING FORK TESTS
There are two main tuning fork testing methods: the Rinne
and Weber tests. Look to my simpleton
drawings that illustrate these concepts.
Weber Test:
The Weber tests for side of involvement. The vibrating tuning fork is placed in the
middle of the patient’s forehead. Other
options: the fork can be placed between the eyes on the nasal bridge or on the
upper two front teeth (the incisors), depending on the doctor’s fancy or
peculiarity or idiosyncrasy or overall weirdness-in-general. With normal hearing or hearing loss that is
equal in both ears, you’ll hear the sound of the tuning fork pretty much in the
midline or in front of you where the fork is placed. This is due to sound travelling from the
fork, through the air equally to both ears.

However, if say your left ear has diminished hearing, you’ll
hear the sound in your better hearing right ear. This intuitively makes sense (I hope) since
sound will be louder in the better hearing ear.
Your brain interprets this as hearing it in only one ear, even if the
worse ear still can pick up the sound signal.
It happens that the sound perceived by the better ear cancels out what
might be heard in the poorer ear with this test. This is the case if your left ear has a SNHL.

However, if you have a CHL in the left ear, the sound will
be heard in the LEFT EAR. Yes, I did not
stutter; you will hear it in the impaired left ear. Let me explain.

In the case of CHL, the sound travels through the bone of
your skull to directly stimulate the cochlea (which is incased in bone, in
fact, the hardest bone in the body), thereby bypassing the TM and ossicles
completely. Yes, sound travels through
bone, where molecular forces are transmitted from one molecule to the
other. You can hear sound transmitted
through your skull, no matter how dense you’ve been told it is.
This is called bone conduction. Air conduction is the normal means which
sound is picked up by the ear; i.e. sound energy travels through the air to
strike the TM. Since the TM and/or
ossicles are impaired, sound travelling via air conduction is impaired,
and the sound travelling via bone is louder than that travelling by air. Since the cochlea on the affected ear is
directly stimulated through bone, this is heard more loudly air conduction
sound received by the opposite normal ear, and the reason you’ll hear the Weber
test in your poorer hearing ear.
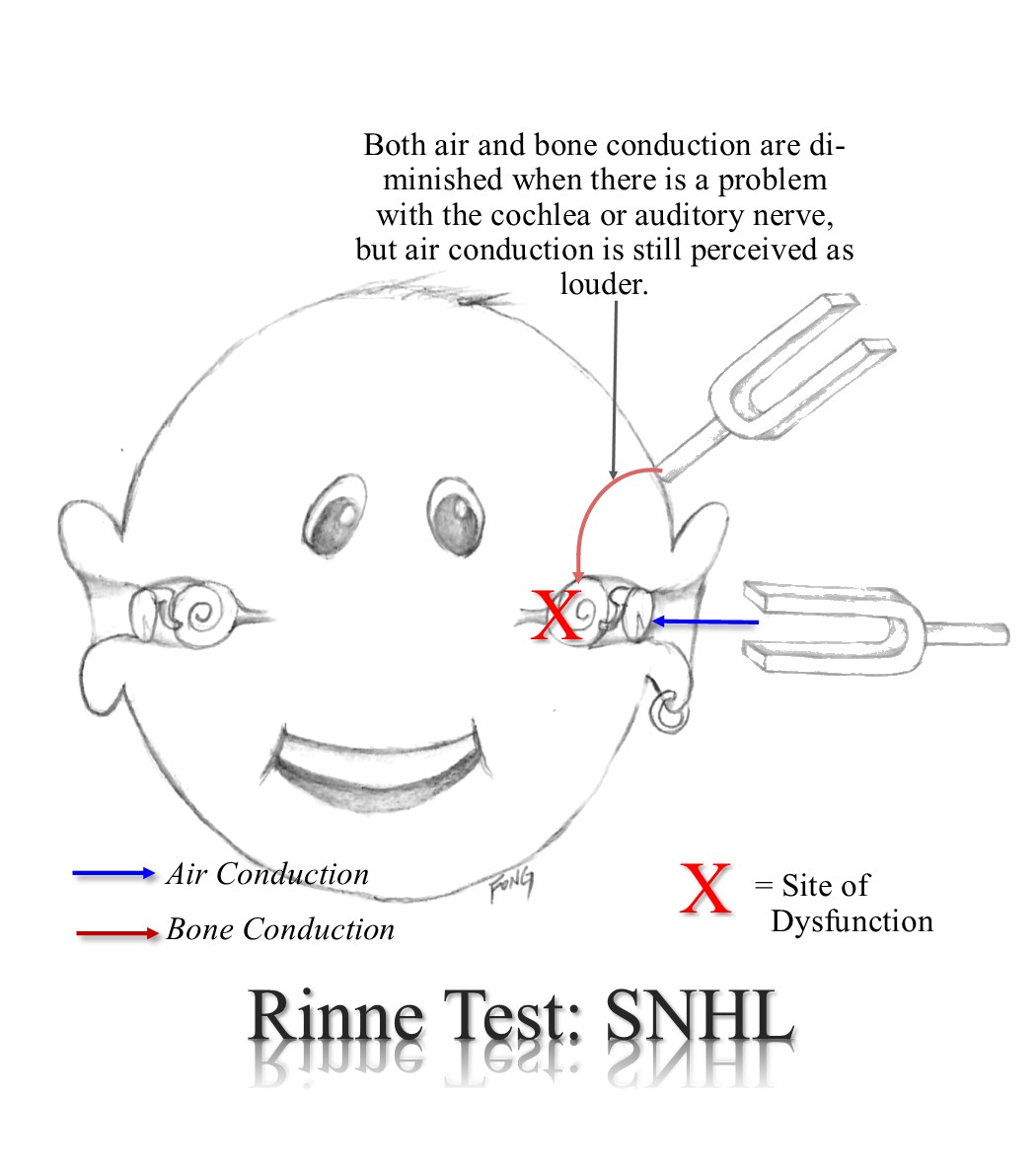
The Rinne Test:
The Rinne test is done by placing vibrating fork first next
to the ear canal (entrance to the ear) but not touching the ear itself. This is the normal way sound is delivered to our
ears. Then the fork is placed behind the
ear onto the skull, to transmit the sound into the skull. You are than asked which sounds louder. This Is another test of air and bone
conduction. To simplify things, I
usually call he air conduction test “number one” and the bone conduction test
“number two,” asking the patient, “Which is louder: number 1 or number 2?” as I
place the vibrating fork 1st near the ear canal and afterwards onto
the skull behind the ear.

If the patient says “number one is louder,” then he/she
hears the sound louder with air conduction.
In this case air conduction is louder than bone conduction and indicates
either normal hearing or there’s a not so severe SNHL. If the response is “number two is louder,”
this indicates a CHL. If you can’t hear or
barely hear the tuning fork with either bone or air conduction, this is a sign
of a very severe SNHL or complete deafness for that ear.
By combining the results of the Weber and Rinne tests, one
can derive a pretty good idea of type of hearing loss that might be
present. For instance, if you hear the
Weber test in your right ear and the Rinne shows bone conduction is louder than
air conduction, this is a good indicator of a CHL in your right ear. If the Weber is heard in the left ear and the
Rinne testing in both ears shows air conduction is louder than bone conduction,
then you’ll have a left SNHL.

If the Weber is heard in the left but the Rinne is equivocal
in the right (i.e., you can’t tell if air is louder than bone conduction) then
you might have a mixed loss in the right ear.
Of course, if you have a severe MHL in one ear with a
substantial SNHL, the Rinne in that ear might reveal reduction in both air and
bone conduction, since the cochlea or auditory nerve is so impaired that it is
difficult to pick up sound by direct cochlear stimulation through bone. Other degrees of MHL however can give
different results, making the tuning fork exam even more confusing in such
cases. This is where more accurate
testing is needed with elaborate equipment as I mentioned above, with an
audiometer, a tympanometer (device that measure TM movement) and a qualified
audiologist (one specifically trained in hearing testing using these
devices).
So relax if you ever see your doc taking out the ominous
appearing tuning fork, and thank God you’re not strapped to the chair with duct
tape over your mouth to silence your screams.
©Randall S. Fong, M.D.
Thanks For sharing very helpful information
ReplyDeleteVibrating Fork Level Switch for Solids